Health inequalities: through a gender lens
In all European countries, social inequalities in health remain high. A wide body of research has highlighted various social factors that affect health. However, gender, as a system of power relations between women and men, is rarely considered as a key determinant of health inequalities. The purpose of GENDHI is to understand how gender intersects with other social relations systems of power relations, such as class and race (racism), to construct social inequalities in health, throughout the life course.
The research is structured around two interrelated questions:
- How are (un)healthy bodies socially constructed?
- Are the uses of the health care system and the care it provides different according to gender?
Women’s advantage in life expectancy (80.5 years for women at birth versus 73.8 years for men in 2016 in Europe), in contrast to what is observed in other social spheres (political, professional, family) has diverted scientific attention from gendered analysis in health. Two main approaches are generally proposed to explain the observed differences between women and men. On the one hand, biological perspectives focusing on genetic, hormonal or immunological dimensions are highlighted as the main determinants of sex differences. On the other hand, social approaches that emphasize the influence of different determinants and representation (tobacco, alcohol, diet, physical activities, professional exposures, etc.) on health, rarely consider gender as part of the social structure of power relations. Although both approaches provide information on the processes leading to differences between men and women, they have, to our knowledge, never been integrated into a comprehensive and theoretically grounded model that allows for a systematic investigation of gender-related health processes over the life course in relation to other social factors of health such as social class and “race”.
The purpose of our project is to provide a multidisciplinary approach to understanding how gender, as a binary system of hierarchy and representation between the sexes (men/women), contributes to the production of (un)healthy bodies and differential health care responses, which in turn informs health inequalities between men and women over the life course.
General purpose and assumptions
Our goals are to explore the “gendered embodied health” and the “gendered health care cascade” by drawing on lifecourse, socialization, and intersectionality approaches.
The life course perspective is a heuristic approach to understanding how social inequalities in health are constructed. It is essential in our project since we start from the assumption that gender does not necessarily play the same role across the life course and within the care trajectory. In this perspective, we distinguish two main stages:
- Firstly, the “gendered embodied health”, refers to the processes that construct (un)healthy bodies, from birth to the end of life, and how we are exposed to various risk factors, including work-related health.
- Secondly, the “gendered health care cascade”, encompasses the perception of symptoms, access to the health care system, diagnoses, treatments, and finally medical follow-up and compliance.
To address our two specific objectives, we draw on two theoretical approaches: (i) intersectionality and (ii) socialization.
(i) Building on the pioneering work of Crenshaw (1989), researchers have formalized the interactions between gender and social class and “race” through the concept of intersectionality. We will question the status of these different social relations and the primacy of gender relations with respect to biological differences between the sexes and the strongly gendered socialization to health
(ii) An intersectional approach allows for an understanding of the complex links between the social and the biological as they relate to classical sociological questions about how society and social structures construct individual bodies through lifelong socialization processes. Socialization processes can be defined as processes by which people are “constructed” or even “conditioned” by society, and thus “learn”, “incorporate” or “integrate” ways of doing, thinking and being that are socially situated and specific to the society in which they find themselves (Darmon, 2023 [2006]). While the body is always present, explicitly or implicitly, in gender socialization approaches, very little work has been done on health within this approach. Therefore, socialization studies on health behaviors (diets, tobacco or alcohol consumption, physical exercise), psychological vulnerability, social participation, and relationships to time and the future, as they relate to health, still need to be developed to understand how gender socialization processes can explain health conditions. We consider that educational styles, somatic sensations, pain management and relations with (medical) institutions, or other health-related activities and attitudes, must also be taken into account in this perspective.
We will put the sociological approach of “socialization” in perspective with that of “embodiment” as it has emerged in epidemiology. The concept of embodiment refers to “the way in which we literally, biologically incorporate the material and social world in which we live” (Krieger 2001). In this way, individuals come to physically incorporate their past environments through a continuous process of change (Kelly-Irving and Delpierre 2018). This approach is also closely related to the observation of the evolution of the social gradient in health over time and age, which is a classic approach in the economic analysis of socioeconomic inequalities in health (Case et al. 2002; Apouey and Geoffard 2013, 2014).
Conceptual model
The Gendhi model provides a dynamic analysis of the social production of health inequalities. Firstly, it is the result of several interconnected stages, namely health outcomes, symptom perception and healthcare. Secondly, individuals’ health trajectories at a given point in time are influenced by their previous health experiences.
The model posits that living and working conditions primarily determine health. Beyond direct health exposures, these material conditions are incorporated into socialisation processes, through which individuals learn and acquire ways of thinking, feeling and acting throughout their lives. This includes somatic sensations and ways of interacting with health professionals, for example.
The Gendhi model then examines a key stage that can influence healthcare utilisation: the perception or non-perception of symptoms. When faced with a health problem, some people may not experience any symptoms, while others may experience symptoms late or not interpret them as a health problem. This can delay recourse to the healthcare system. However, these feelings vary according to gender, race and social class. The model then examines inequalities in access to healthcare and treatment, with a particular focus on interactions between patients and healthcare professionals, as well as professional practices.
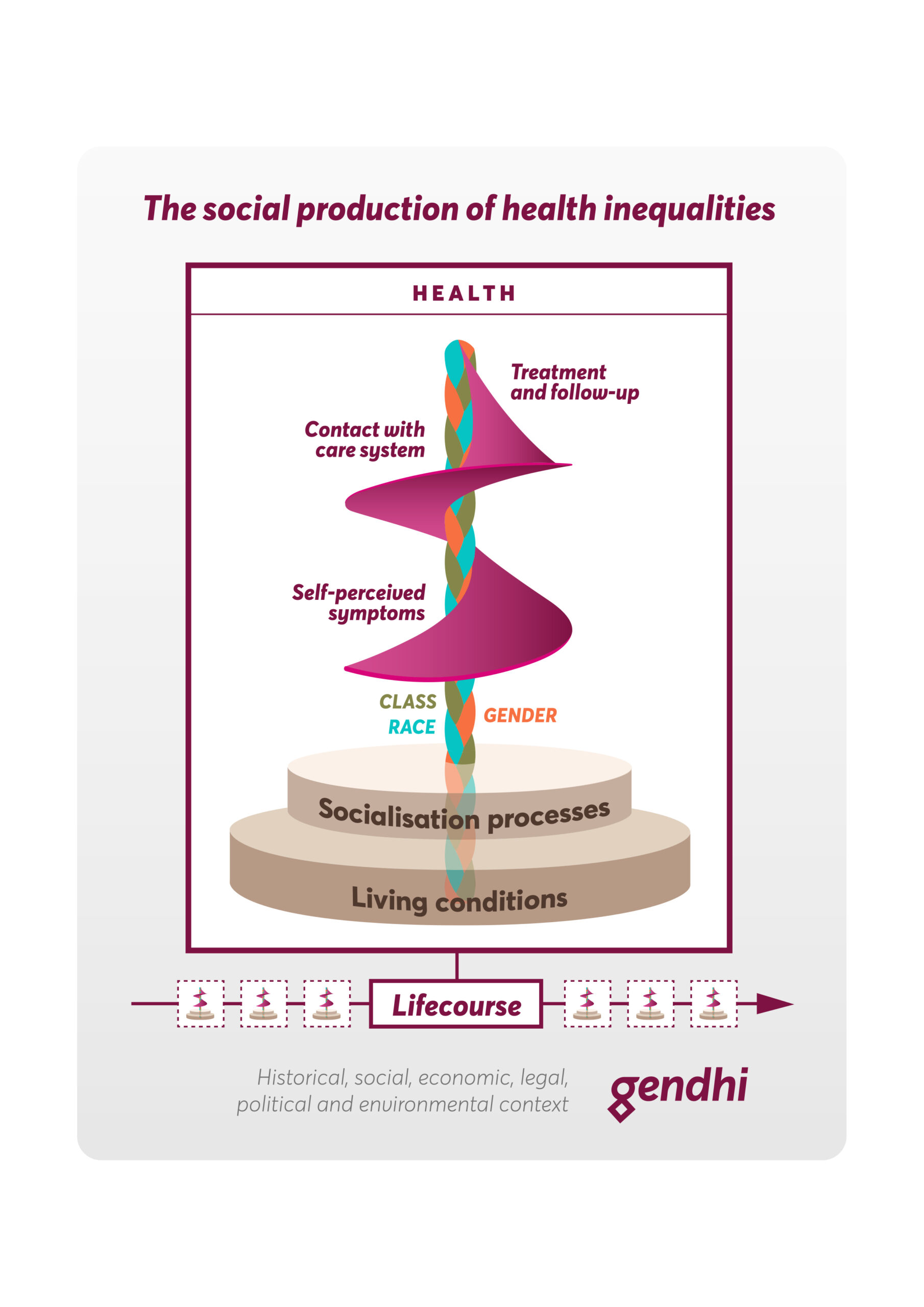
Fig. 1. Social production of health inequalities : Conceptual model
Methodology
We will use a mixed-methods approach, including quantitative analysis of large cross-sectional and longitudinal datasets and innovative qualitative research, providing specific and complementary perspectives on the interrelationship between gender and health and the ability to triangulate our findings to strengthen our conclusions. In order to integrate qualitative and quantitative perspectives, we focus on one country, France, to test our theoretical model empirically.
Our research program combines quantitative (multiple correspondence analysis, hierarchical ascending classification and regression models) and qualitative (family and hospital ethnographies, interviews, observations) methodologies.
Our proposed original theoretical framework is being used to examine:
- existing data to carry out quantitative analysis of 6 large datasets and epidemiological cohorts (Elfe, SHARE, Constances, HBSC, ESS, Epicov)
- original materials consisting of family monographs (repeated interviews with parents and children), interviews with young people in secondary schools, interviews with patients and health professionals, ethnographies of hospital services and observations of medical consultations, as well as a critical analysis of medical recommendations.
The approach is resolutely multidisciplinary, combining sociology, demography, economics and epidemiology, in close collaboration with clinical researchers.
We have focus on four diseases types that are widely prevalent in Europe: cardiovascular pathologies, depression, colorectal cancer, and COVID-19, as well as ageing-related processes over the life course. These health outcomes were chosen on the basis of gender differences in diagnosis (underdiagnosed myocardial infarction in women, underdiagnosed depression in men, presence or absence of biomarkers in diagnosis) and gender differences in treatment (hypertension, myocardial infarction) or mortality (COVID-19, ageing).
The gendered cascade of medical care
The gendered health care cascade will be studied from the experience (or lack thereof) of symptoms, through diagnosis, prescriptions and compliance (or lack thereof), to hospitalization and its consequences. Current medical guidelines are being analysed from a gender perspective through a textual analysis of documents from European academic societies (cardiology, psychiatry, neurology and oncology). Gender-specific pathways to and through the health care system are being examined usng date from the Constances cohort.
For each of the five conditions, we will reconstruct the health care cascade: starting with the expression of symptoms, moving to medical consultation and subsequent diagnosis, and ending with treatment and compliance. To observe the gendered nature of doctor-patient interactions and how gender shapes medical decisions, we will conduct an ethnographic analysis of services specializing in the management of the conditions under study and conduct retrospective interviews with men and women for each condition.